
Part1
A disease of dis-ease, the day a young girl starts her journey of reproductive life ,a dilemma leading to pathologies till the fecundity decline.
In history characteristics of disease described at least as far back as 1600 BCE. Schrön described a “female disorder in which ulcers appear in the abdomin, bladder, intestines and outside the uterus and cervix, causing adhesions”. First histological description credited to Von Rokitansky.
Cullen later suggested endometriomas (“adenomyomas”) resembled mucous membrane of uterus and Sampson generally credited for providing first theory on pathogenesis; coined term “endometriosis” in 1921.
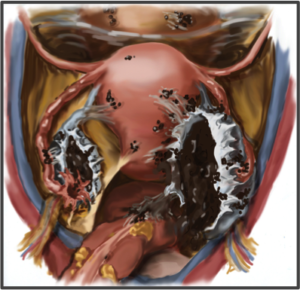
Clinically defined as presence of endometrial-like tissue found outside uterus, resulting in sustained inflammatory reaction, an estrogen-dependent disease frequently resulting in substantial morbidity, severe pelvic pain, multiple surgeries, and impaired fertility.
A leading cause of gynecologic hospitalization and hysterectomy with efficacious treatment requires multidisciplinary approach and corresponds to high association of co-morbid conditions.
“Disease of theories”; definitive causes remain under debate, though associations with number of hereditary, environmental, epigenetic, and menstrual characteristics affecting 176 million women globally, 70% of teens with pelvic pain are later diagnosed with endometriosis. Symptoms are wide-ranging as early as 8 years of age, high rates of disease may be underappreciated by medical and lay communities and may be indicative of possible future endometriosis in adolescents and young women .
 Symptoms depend the area and extent of involvement of disease.e.g
Symptoms depend the area and extent of involvement of disease.e.g
- Painful periods (dysmenorrhea) with or without heavy or irregular bleeding
- Cylical/noncylical pelvic pain
- Lower abdominal or back pain
- Often with cycles complain of diarrhea/constipation Bloating, nausea, and vomiting
- Inguinal pain
- Painful micturation(Dysuria)
- Painful sex(Dyspareunia) .
- Nodules may be felt upon pelvic exam
- Imaging may indicate pelvic mass/endometriomas
- Inverse BMI relationship
The economic burden from both a sufferer’s and societal perspective is profound. Recent data shows $119 billion annually can be attributed to the disease with significant loss of productivity: 11 hours per woman per week; 38% more than for women with similar symptoms without endometriosis.
Per-patient cost increased 61%; adolescents (aged 10−17 years) had endometriosis-related hospitalizations; approximately 50% of >600,000 endometriosis-related ambulatory patient visits involved specialist care; and females 23 years old or younger constituted >20% of endometriosis-related outpatient visits., 63% higher than medical costs for the average woman in a commercially insured group.
72% reported having eight or more endometriosis-related or coexisting symptoms, interfered with their daily life and work activities. 85% of respondents noted a decrease in quality of their work and almost 20% reported being unable to work due to pain, while 69% reported otherwise.
40% of patients perceived that, their career growth was negatively affected due to high rates of absenteeism and/or low performance, not being promoted, not receiving merit/excellence bonuses, missing professional seminars, and loss of clients. Others reported being “totally incapacitated” and dismissed from or quit their jobs due to symptoms.
 DIAGNOSIS:
DIAGNOSIS:
- Clinical Diagnosis:
- Pelvic Examination & Pain Mapping
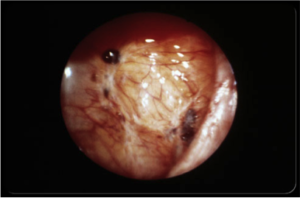
- Imaging Studies
- Surgical Diagnosis & Staging
Due to lack of awareness, endometriosis is an often underappreciated diagnosis. Women and girls with the disease suffer a delay in diagnosis, on average, of 7 to 12 years and may present to five or more physicians before their pain is addressed. Moreover, the disease may be mistakenly dismissed as routine menstrual pain, particularly in younger women.
Physical examination has poor sensitivity, specificity, and predictive value in the diagnosis of endometriosis. When probed, the patient may exhibit pain. A thorough combination of history, physical examination, and laboratory and additional diagnostic studies as indicated must be done to determine the cause of pelvic pain and rule out other non-endometriosis concerns.

About Author:
Dr. Asma Munir Ur Rahman
Specialist B Gynaecologist and Obstetrician